Effect of crack length on crack enlargement during convection-enhanced nanofluid delivery in tumors
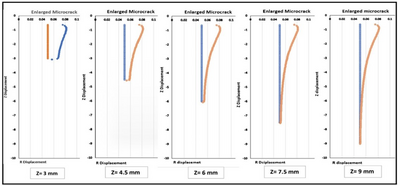
In nanofluid delivery, backflow along the needle is a major hurdle to deliver drug-carrying nanofluid to the entire tumor. In theory, any approaches to decrease the overall flow resistance in tumors would facilitate drug delivery. The objective of this study is to develop a theoretical approach to improve the depth of nanofluid penetration in tumors via introduction of a microcrack. We perform theoretical simulations to evaluate how the introduction and enlargement of a microcrack in tissue reduces the overall flow resistance in the porous tumor during convection-enhanced delivery (CED). Both Darcy’s law and the theory of poroelasticity in the Sub-surface module in COMSOL are used in the simulation to understand the fluid transport in a 20 mm diameter spherical tumor with or without microcrack introduction and/or enlargement. We assume that a cylindrical microcrack with a diameter of 0.05 mm and length varying from 3 mm to 9 mm is introduced by a retractable needle at the tumor center. Nanofluid is then infused at the center of the tumor and flows to the tumor periphery. Both regions are porous media, with the permeability of the microcrack much bigger than that of the tumor. With an infusion pressure at 210^5, one finds significant lateral deformation in the crack, however, the deformation tapers along the microcrack to change its shape from the original cylinder to a frustum. The deformation of the microcrack is reconstructed using EXCEL. The maximal lateral deformation of the microcrack is approximately 0.037 mm, resulting in doubling the volume of the original microcrack. As shown in the figures, the effect of microcrack enlargement significantly subdues in the axial direction. It suggests the diminishing influence of the fluid pressure that restrains further expansion along the microcrack. After importing the enlarged microcrack back to COMSOL, one can simulate the pressure distributions in the vicinity of the microcrack. The updated pressure field illustrates that a longer microcrack extends the maximal isobaric pressure contour towards the tumor periphery. In this study, we also simulated the velocity field inside the porous tumor to determine the volumetric flow rate at the tumor outer surface. Without the microcrack, the total flow rate is 8.5910^(-10) m^3/s. Since the microcrack has a very large permeability, with the initial microcrack length of 3 mm, the enlarged microcrack would significantly increase the total flow rate to 1.00210^(-9) m^3/s. Further lengthening the microcrack to 9 mm results in an increase to 1.03410^(-9) m^3/s. The flow resistance defined as the infusion pressure divided by the total flow rate, decreases significantly. Introducing the microcrack alone without deformation shows up to 10% in the resistance reduction, while with a deformed microcrack, the total resistance decreases by 17%. We conclude that introducing a microcrack into porous tumors is an effective strategy to enhance fluid flow and, consequently, the distribution of therapeutic agents using CED. By reducing flow resistance and facilitating a more uniform dispersion of drugs, microcrack formation and enlargement is a promising technique for improving the efficacy of cancer treatments.